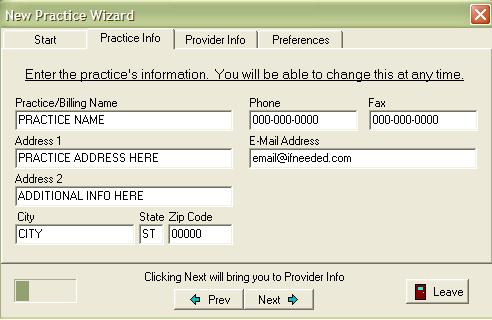
- Practice Name - The name of your practice.
- Address 1 - The street address/post office box of your practice.
- Address 2 - Any additional address information.
- City - City where you practice is located.
- State - State where you practice is located
- Zip - Zip code in which your practice is located.
- Phone - The telephone number of the practice.
- E-mail Address - The E-mail address of you practice (if applicable).
- Tax ID - The Federal Employer Number assigned to your practice (if any); otherwise, use social security number.
|
|
|